Pharmacodynamics is made up of two words “Pharmakon” means drugs and “Dynamic” means power. So, we can say the Pharmacodynamic means power of drugs or what the drug does to the body.
Pharmacodynamic is a part of pharmacology in which we study the:
- Biological effects of a drugs
- Mode of drug action (how it acts?)
- Therapeutic effects
- Side/toxic effects
- Relationship between drug concentration and biological effects.
Principles of Drug Actions
Generally, drugs (except gene modifiers) do not produce any new biological action they just alter the pace of ongoing physiological function like
- Stimulation: Enhance cellular activity. E.g., Adrenalin increases the heart rate. But sometimes it may be dangerous like Picrotoxin is a CNS stimulant which may cause convulsion or coma.
- Depression/Inhibition: inhibition of activity. E.g., Barbiturates decrease the CNS activity, acetylcholine reduces the heart rate.
- Irritation: Noxious effects or counter-irritant. E.g., bitter drugs increase salivation.
- Replacement: Replace in deficient condition. E.g., hormone replacement therapy, L-dopa in Parkinson’s therapy.
- Cytotoxic Effects: Cell killing action. E.g., Anti-cancer drugs kill the cancer cells, antimicrobial agents kill the infective agents.
How do Drugs act?
Paul Ehrlich proposed that ‘Corpora non-agunt nisi fixata’ which means a drug will not work unless it is bound to the cellular targets. As per these concepts, a drug-protein complex is necessary to biological actions.
Drugs—Drug-protein complex—Signal transduction—Cellular response
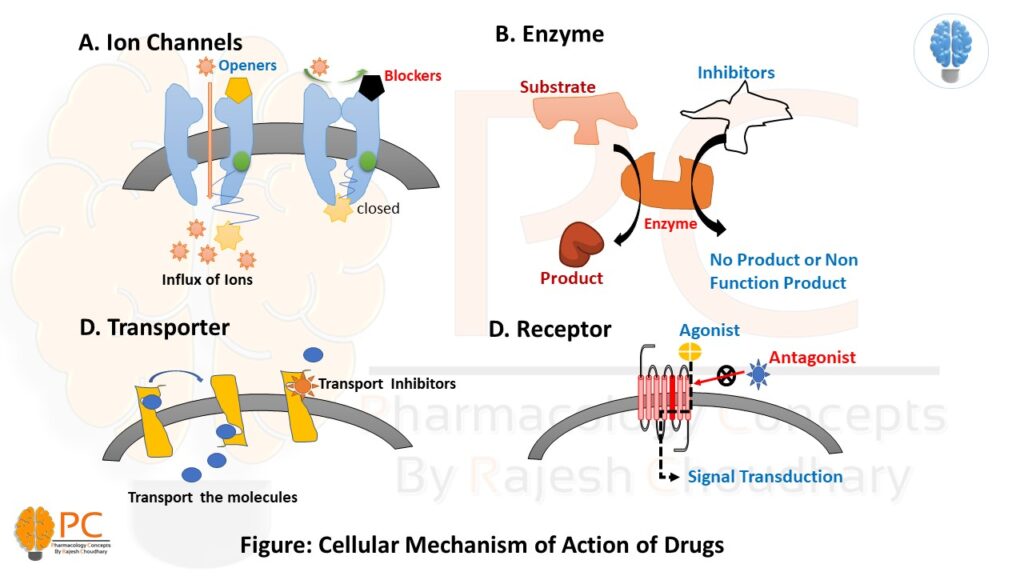
The major cellular target proteins are:
- Ion Channels
- Enzymes
- Transporters
- Receptors

1. Ion Channels-based drug action
The cells contain a variety of ion channels like Voltage-gated ion channels (VGIC: Na+, K+, Ca2+, and Cl-), Ligand gated ion channels (LGIC) and G-protein operated ion channels (GpOIC). The LGIC and GpOIC are part of receptor-based drug actions. Some drugs directly affect the VGIC and show their biological action.
- Quinidine blocks myocardial Na+ channels.
- Dofetilide and amiodarone block myocardial delayed rectifier K+ channel.
- Nifedipine blocks the L-type of voltage-sensitive Ca2+ channel.
- Nicorandil opens ATP-sensitive K+ channels.
- Sulfonylurea hypoglycaemics inhibit pancreatic ATP-sensitive K+ channels.
- Amiloride inhibits renal epithelial Na+ channels.
- Phenytoin modulates (prolongs the inactivated state of) voltage-sensitive neuronal Na+ channel.
- Ethosuximide inhibits T-type of Ca2+ channels in thalamic neurons
2. Enzyme-based drug action
Some drugs either activate or inhibit the catalytic activity of an enzyme and alter the ongoing pathophysiological process.
A. Enzyme Stimulation: enzyme activity stimulation increases its affinity for the substrate so that the rate constant (kM) of the reaction is lowered
- pyridoxine acts as a cofactor and increases decarboxylase activity
- Adrenaline stimulates hepatic glycogen phosphorylase
B. Enzyme Inhibition: some drugs inhibit the enzyme activity and decrease the production rate or produce inactive or false products.
- Nonselective Inhibitors: heavy metal salts, strong acids and alkalies, formaldehyde, and phenol denatured the protein and inhibit the enzyme activity.
- Selective Inhibitor: some drugs selectively inhibit a specific type of enzyme in a competitive or non-competitive manner.
A. Competitive inhibitors: They are structurally similar to substrate thus competitively inhibit the enzyme activity. They generally increase the Km value but Vmax remains unchanged. E.g., physostigmine inhibits the cholinesterase, sulfonamides inhibit the dihydrofolate synthetase.
B. Non-Competitive inhibitors: They bind to the adjacent sites or allosteric sites and inhibit enzyme activity. Due to binding to the adjacent site, they decrease the Vmax but Km remains unchanged. E.g., Acetazolamide inhibits carbonic anhydrase, Aspirin inhibit the COX enzyme, and Digitoxin inhibits the Na+K+ATPase

3. Transporter-based drug action
Transportation or translocation of several drugs or biomolecules requires a specific transporter (Facilitate diffusion and active transport system) to across the cell membrane, and some drugs modulate these transport systems and interfere with the translocation.
- Norepinephrine transporter (NET) is inhibited by desipramine and cocaine
- serotonin transporter (SERT) is inhibited by Fluoxetine (and other SSRIs)
- Dopamine transporter (DAT) is inhibited by Amphetamines
4. Receptors
The largest number of drugs act through specific regulatory macromolecules (located at the cell surface of intracellular) which control the above effectors (Enzymes, Ion Channels, and Transporters). There are cellular targets or regulatory macromolecules called Receptors. Some drugs (Agonists) activate this receptor and forward the biological response while some drugs (Antagonists) block this receptor and prevent its activation.
The details of receptor pharmacology will be explained in another blog post.
Examples of biomolecules and their receptor are:
- Muscarinic Receptor – Acetylcholine
- Alfa/Beta receptors- Adrenaline
- GABA Receptor- GABA, Barbiturates, Benzodiazepines
*But besides these, the drug may also show their action by their physical and chemical properties.
5. Physical property-based drug action:
- physical mass- Bulk laxatives (ispaghula)
- Adsorption property- Activated charcoal
- Radiation (UV) absorption- Para amino benzoic acid
- Osmotic diuretics- Mannitol
- Radioactivity- I131
6. Chemical Properties-based drug action:
- Antacids—the neutralization of gastric HCl
- permanganate—oxidizing property
- Chelating agents (EDTA, dimercaprol)—chelation of heavy metals.