Drug excretion is defined as the irreversible loss of drug molecules or their metabolites from the body. Drugs are excreted through the body. Drugs are excreted from the following routes:
- Urine (Renal Excretion): most of the drugs and metabolites.
- Feces (Biliary Excretion): unabsorbed fraction of drugs and having a large molecular weight (>300 D). e.g., Corticosteroids, heavy metals.
- Exhaled Air (Lungs): volatile liquid or gases. E.g., Inhaled general anesthetics, alcohol, paraldehyde.
- Salivary Excretion: Some drugs excreted through saliva like Li, KI, Heavy metals, Rifampicin.
- Milk Excretion: some drugs are secreted into breast milk like lipid soluble drugs (basic in nature).
RENAL EXCRETION
Most of the drugs and their metabolite are excreted through urine. Therefore, the kidney is considered a major excretory organ. Drugs and metabolites are excreted from the kidneys by two ways: Glomerular filtration and Tubular secretion, however from the Tubular reabsorption lipid fraction of the drugs or lipid drugs are reabsorbed thus tubular secretion is not involved in drug excretion but affect the net content of excretion.
Renal Excretion = (Glomerular filtration + Tubular secretion) – Tubular reabsorption
Renal Clearance = Urine volume (ml)/Time (min)
Renal clearance indicates how much urine (volume in ml) is excreted per unit time (min) but drug excretion mainly depends on the amount of drug eliminate through urine. So, the rate of renal excretion (RE) indicates the amount of the drug present in the urine which excreted per unit time.
Rate of renal excretion (RE) = mass (mg)/time (min)
Renal Clearance = Volume/Time
Renal Clearance = RE/plasma concentration
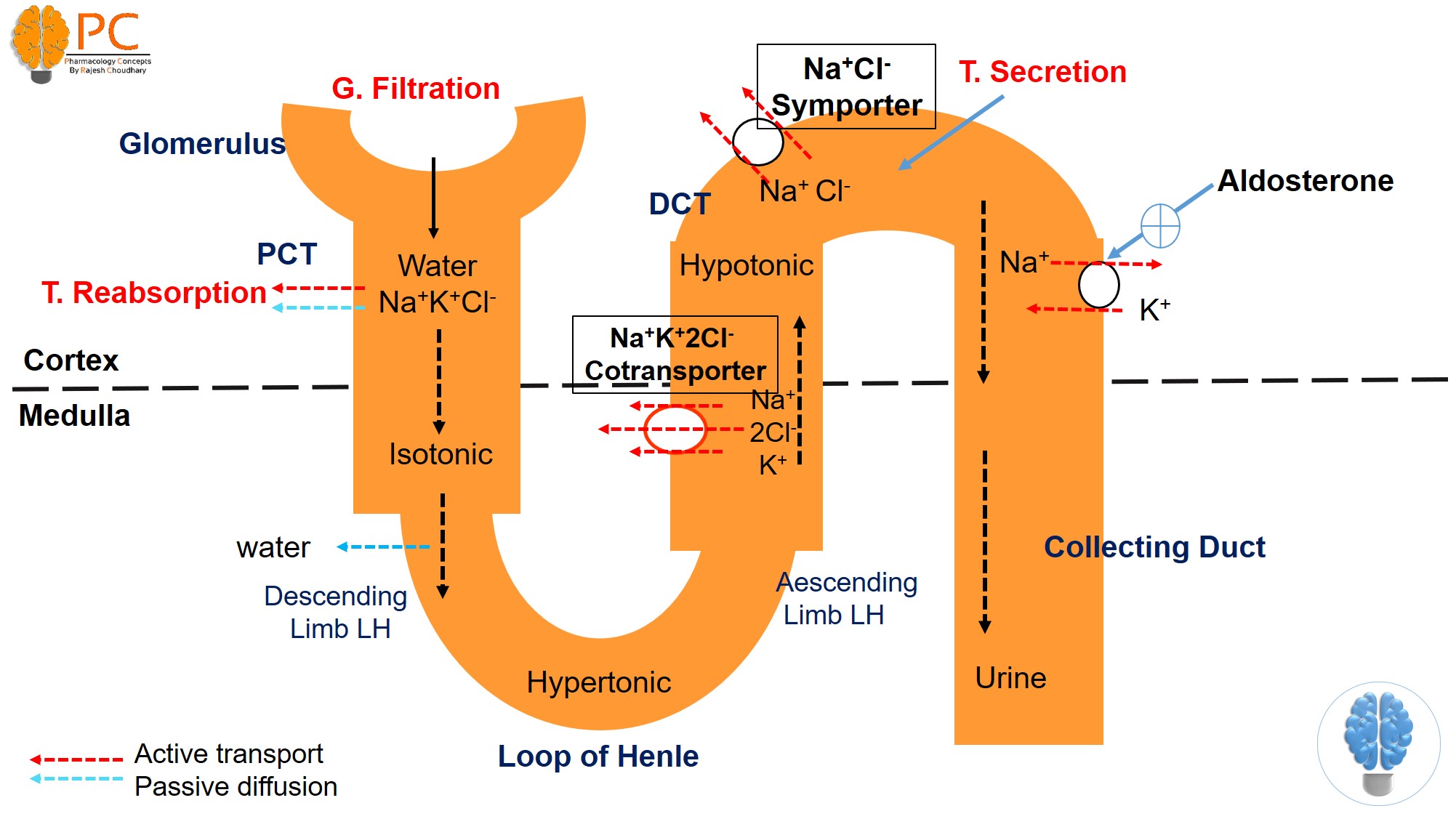
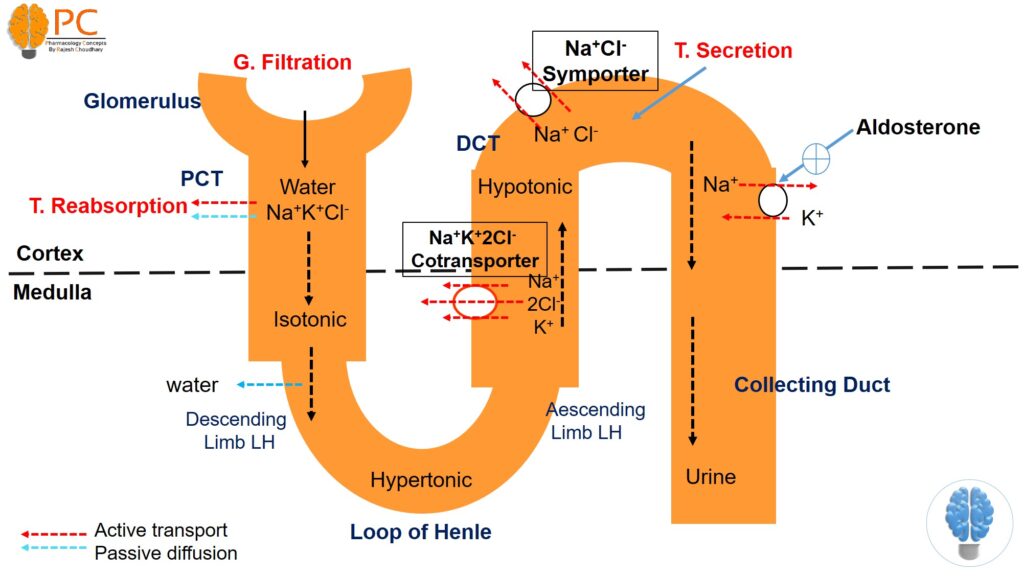
Figure 1. Renal excretion of drugs
There are four important factors that affect the renal clearance of the drugs:
- Plasma protein binding of the drug.— ——-decrease
- Tubular reabsorption ratio of the drug.——decrease
- Tubular secretion ratio of the drug. ———–increase
- Glomerular filtration ratio of the drug.——-increase
- Glomerular Filtration
- Simple passive diffusion play role in glomerular filtration.
- In the glomerular filtration, only free drugs are filtered from the glomerulus into proximal tubules while the bound fraction of drug molecules (plasma proteins bounded drugs) are not filtered. Because albumin (plasma protein) cannot be filtered from the glomerulus, the drugs cannot pass through into the proximal tubules.
- The filtration rate is approx. 110-130 ml/min.
- Standard GFR = 120 ml/min = Creatinine Clearance
- GFR can be monitored by Creatinine or inulin.
- GFR decreases with aging (>50 y) or renal failure. It can cause the reduction or elimination and may precipitate drug toxicity.
- Tubular Secretion
- Tubular secretion occurs mainly in the proximal tubules. The protein bounded drugs are dissociated in PCT and excrete via T. secretion. Active transport is the main mechanism for tubular secretion. There are two types of active transport systems Anionic transport (OAT) and Cationic transport (OCT).
- Anionic transport (OAT)- for acidic drugs (Pencilline, probenecid, salicylate, MTX). And Cationic transport (OCT)- for basic drug (Thiazides, quinidine, procainamide, cemitidine).
- Due to specific active transport system displacement interaction is occurs, which means two drugs compete with the same transport system and thus one drug reduce the tubular secretion of another. E.g. probenecid decreases the T. secretion of penicillin thus reduce the elimination and increase the duration of action.
- In neonates, the transport system is not fully developed, therefore, the elimination of certain drugs is reduced and enhances the duration of action.
- The efficiency (performance) of the excretion by tubular secretion is higher than the glomerular filtration route. The clearance maximum in glomerular filtration is approximately 120 ml/min, whereas the clearance maximum of tubular secretion is about 600 ml/min.
- Tubular Reabsorption
- Most (90%) of the lipid drugs .
- Tubular reabsorption occurs mainly in distal tubules and partially in proximal tubules.
- It occurs by simple passive diffusion generally
- Changing the pH value of the urine (making the urine acidic or basic) is going to change the ionization degree and the simple passive diffusion of the drug or the metabolite and lastly affect the excretion from the kidney.
- Acidic drugs are mainly excreted in basic urine and basic drugs are excreted in acidic urine
- In the presence of urine acidifiers NH4Cl), excretion of weak basic drugs will increase and reabsorption of the weak acid drug from the renal tubules into the blood will increase, thus the excretion will decrease. So urine acidifiers may be used to eliminate basic drugs like morphine and amphetamine. But clinically, urine acidifying increases the risk of Cardiotoxocity and Rhabdomyolysis.
- On the other hand, in the presence of urine alkalizer (Na2CO3), excretion of the weak acidic drug will increase. Therefore, a urine alkalizer may be used to excretion of acidic drugs (Used in barbiturates or salicylate poisoning)
BILIARY EXCRETION
- Some drugs (highly ionized polar; conjugated product compounds; >500KD) are secreted from the hepatocytes by active transport to the biliary ducts and reach to the intestine. E.g., Steroids, Purgative, Heavy metal.
Enterohepatic Circulation
- Some hepatic drug metabolites are drained to the small intestine to the biliary duct and they are reabsorbed again and reach to the liver by portal vein this cycle is called the enterohepatic cycle
- The enterohepatic cycle may increase the duration of action.
- g., Chlorpromazine, Digitoxin, Indomethacin, Chloramphenicol
ELIMINATION KINETICS
First Order kinetic:
- Constant proportion (50%) of drug eliminated per unit time.
- Rate α Conc.
- Rate= Cl x Conc.
- T1/2 = 0.693/k
- T1/2= constant
- E.g. Most of the drugs.
TIME | DRUG LEFT % | RATIO OF THE DRUG LEFT |
0 x t1/2 | 100 | 1 |
1 x t1/2 | 50 | 1/2 |
2 x t1/2 | 25 | 1/4 |
3 x t1/2 | 12,5 | 1/8 |
4 x t1/2 | 6,25 | 1/16 |
5 x t1/2 | 3,125 | 1/32 |
Zero order kinetic:
- Constant amount of drug eliminate per unit time
- R α Co
- Rate = constant
- T1/2 = 0.5 Conc. / k
- T1 > T2 > T3
- E.g. : (Zero WATT Power)- Warfarin, Alcohol, Theophylline, Tolbutamide, Phenytoin, and Salicylate.
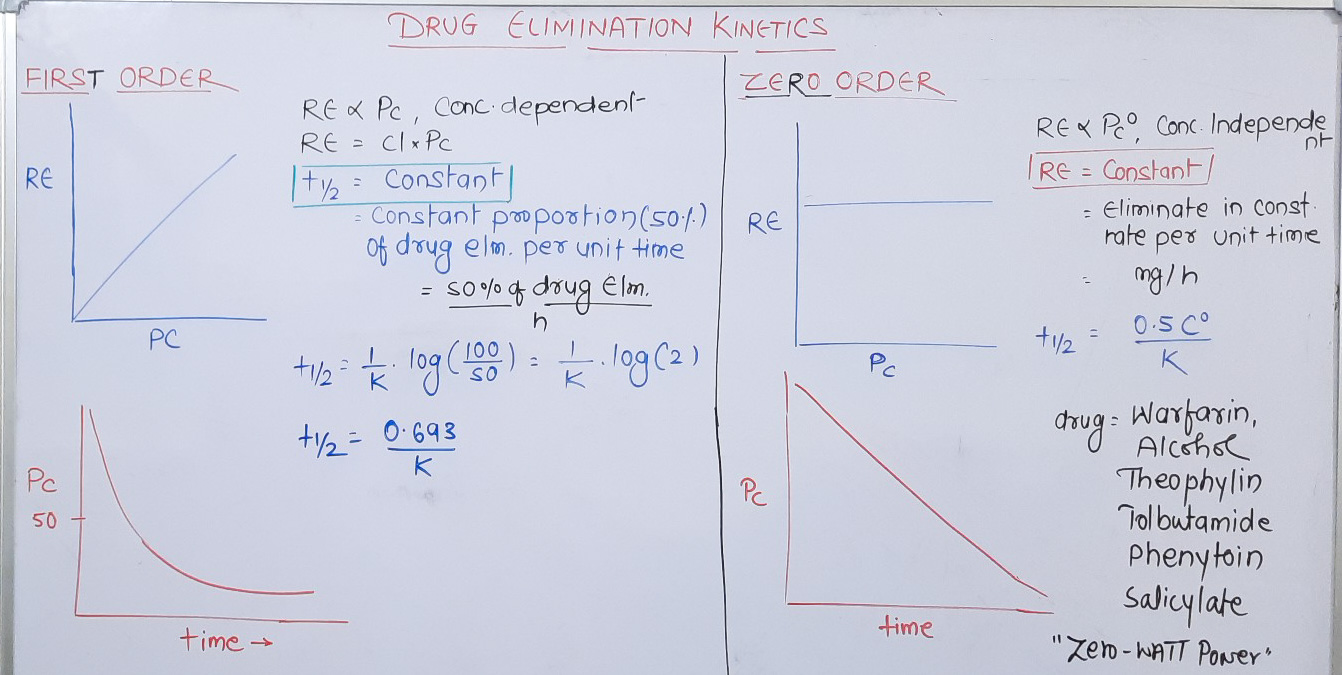
Figure 2: Drug Elimination Kinetics